Fibroids or leiomyomas are extremely common lesions of the uterus. This blog covers if and how it impacts your fertility.

You’ve just been told you have fibroids. Maybe it was during a routine ultrasound, maybe while investigating why you’re not getting pregnant. Either way, you’re sitting there with a thousand questions racing through your mind: Does this mean I can’t have children? Do I need surgery? Should I panic?
Let’s take a breath and talk about what fibroids actually mean for your fertility—because the answer isn’t as simple as “yes, they’re a problem” or “no, they’re fine.” Like most things in medicine, it depends.
What are fibroids?
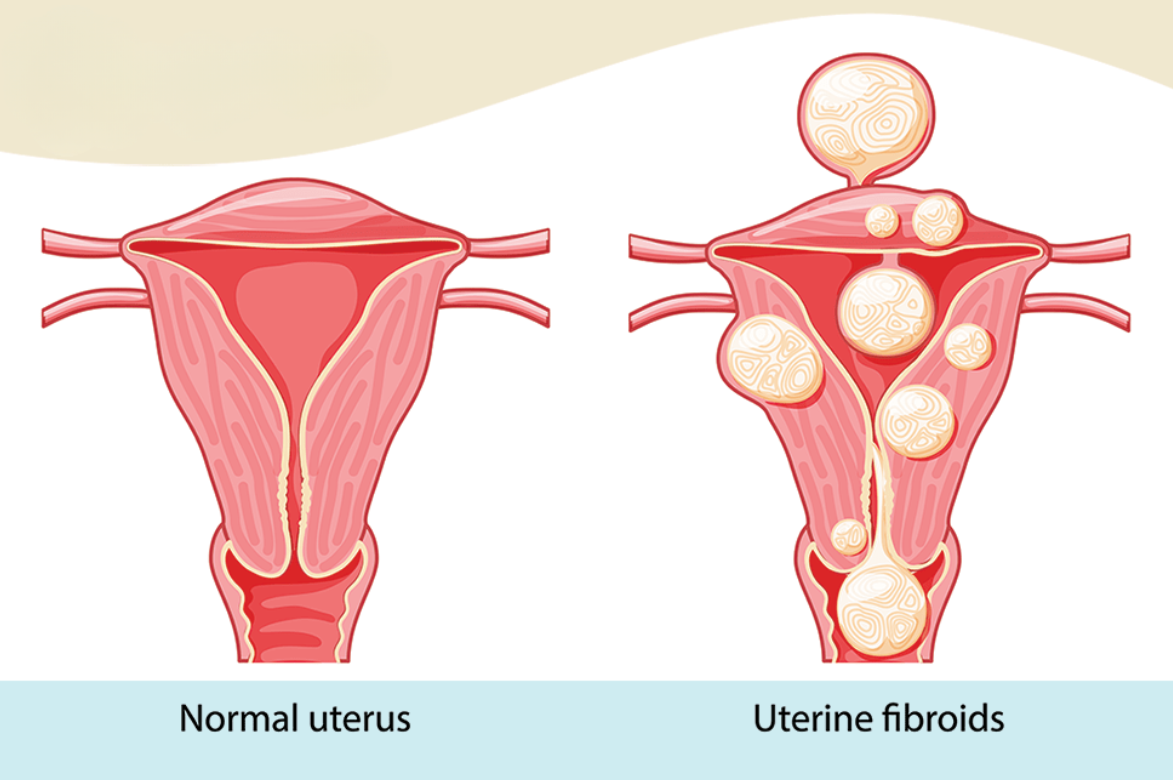
Fibroids, also called leiomyomas or myomas, are benign (non-cancerous) growths made of muscle tissue that develop in or on your uterus. They’re incredibly common—up to 80% of women will develop them by age 50, and they’re especially common during the reproductive years.
Here’s something that might surprise you: most women with fibroids don’t even know they have them. Many fibroids cause no symptoms at all and are discovered accidentally during ultrasounds for other reasons.
Fibroids can be as small as a seed or as large as a melon. You might have one, or you might have several. They can grow slowly or quickly, and they can be located in different parts of your uterus—and that location matters more than almost anything else when it comes to fertility.
The three types of fibroids (And why location is everything)
Not all fibroids are created equal. Where they’re located determines whether they’ll affect your fertility:
Submucosal fibroids grow just under the lining of your uterus and bulge into the uterine cavity (the space where a baby would develop). These are the troublemakers. Even small submucosal fibroids can significantly affect fertility by distorting the uterine cavity and interfering with implantation.
Intramural fibroids grow within the muscular wall of your uterus. These are the most common type. Whether they affect fertility depends on their size and whether they distort the uterine cavity. Large intramural fibroids (especially over 4 cm) can cause problems, but smaller ones that don’t affect the cavity usually don’t.
Subserosal fibroids grow on the outer wall of your uterus, sometimes on a stalk. These rarely affect fertility because they don’t interfere with the uterine cavity or implantation.
The bottom line: The closer a fibroid is to the uterine cavity, the more likely it is to cause fertility problems.
How Fibroids Can Affect Fertility
When fibroids do cause fertility issues, here’s what they’re actually doing:
Changing the shape of the uterine cavity: Submucosal fibroids can distort the space where an embryo needs to implant, making it difficult or impossible for implantation to occur. Think of it like trying to pitch a tent on uneven ground—technically possible, but much harder.
Blocking fallopian tubes: If fibroids are located near the opening of your fallopian tubes, they can physically block the path that eggs need to travel from your ovaries to your uterus.
Affecting blood flow to the endometrium: Large fibroids can interfere with blood supply to the uterine lining, making it less receptive to embryo implantation.
Affecting the cervix: Fibroids near the cervix can change its shape or position, potentially affecting how sperm travels into the uterus.
Here’s what often gets lost in the panic: fibroids are found in approximately one-fifth of sub-fertile women, but they’re also found in many women having no trouble getting pregnant at all.
All this means is, fibroids may cause infertility but only in very specific situations.
Do Fibroids Affect IVF Success?
If you’re considering IVF or have already started treatment, the impact of fibroids depends entirely on their type and location.
Submucosal fibroids that distort the uterine cavity significantly reduce IVF success. Studies show that they can reduce your chances by about 70%.
Intramural fibroids have a more modest effect, with an odds ratio of about 0.7 for implantation and delivery—meaning they might reduce success by about 30%, and mainly when they’re large.
Subserosal fibroids have minimal to no impact on IVF outcomes.
This is why most fertility clinics recommend removing cavity-distorting fibroids before starting IVF.
Treatment Options: What Can Be Done
If fibroids need to be removed, the good news is that there are several fertility-preserving options:
Hysteroscopic myomectomy: For submucosal fibroids, these can often be removed through the vagina and cervix with a camera (hysteroscope). This is minimally invasive, has quick recovery, and doesn’t require any abdominal incisions. There’s no reported risk of uterine rupture in future pregnancies with this approach.
Laparoscopic myomectomy: For intramural and subserosal fibroids, these can be removed through small incisions in the abdomen using a camera and instruments. Recovery is faster than open surgery, and pregnancy rates after laparoscopic myomectomy reach 50-60% with good obstetrical outcomes.
Abdominal (open) myomectomy: For very large fibroids or multiple fibroids, traditional open surgery through a larger incision might be necessary. Pregnancy rates are similar to laparoscopic approach (50-60%).
Recovery and pregnancy timing: After myomectomy, you typically need to wait 3-6 months before trying to conceive, to allow the uterus to heal properly. The exact timing depends on the type and extent of surgery.
Pregnancy and Fibroids
One common worry is whether fibroid removal surgery affects your ability to carry a pregnancy. Here’s what research shows:
Good news: Pregnancy rates after myomectomy range from 50-68%, and most women have good obstetrical outcomes.
Things to know: After myomectomy (especially laparoscopic or open surgery where the uterine wall is cut), there’s a small risk of uterine rupture during labor. Because of this, many women who’ve had myomectomy are advised to deliver by C-section, though vaginal delivery is possible in select cases.
Recurrence: Fibroids can grow back. About 20-30% of women may develop new fibroids after myomectomy, though this depends on factors like age, number of fibroids removed, and genetics.
If you get pregnant with fibroids still in place, here’s what you should know:
Most women have uncomplicated pregnancies: 70-90% of pregnant women with fibroids have no issues related to the fibroids.
Pain can occur: Fibroids can degenerate (die off) during pregnancy as the baby demands more blood supply, which can cause significant pain. This is usually managed with rest, hydration, and pain medication—not surgery.
Slightly increased risks: There may be a small increased risk of miscarriage, preterm labor, abnormal fetal position, or placental problems, but these are not common.
Fibroids usually don’t grow much: Contrary to popular belief, most fibroids remain stable in size during pregnancy (50-60% of cases), with only about 22-32% growing larger.
Ready to Understand Your Fibroids Better?
If you’ve been diagnosed with fibroids—or suspect you might have them—and you’re concerned about your fertility, let’s talk. We offer comprehensive evaluation including ultrasound and, when needed, hysteroscopy to assess exactly how your fibroids might be affecting your fertility.
Book a consultation with us to discuss whether your fibroids need treatment, what your options are, and what timeline makes sense for your family-building goals.
Because not every fibroid needs treatment, but when they do, acting at the right time can make all the difference.